skeletal system

Components : bones , joints and their associated cartilages.
Functions:
· Supports and protects the body
· Provides a surface area for muscle attachments
· Helps body movements
· Houses cells that produce blood cells
· Stores minerals and lipids (fats)
JOINTS

Articulation
of 2 or more bones in a particular region called has a joint
TYPES OF JOINTS
1.
FIBROUS OR FIXED JOINTS

These are
immovable joints have fibrous tissue between the bones example joints between
the bones of the skull and those between the teeth and maxilla and mandible.
2.
CARTILAGINOUS OR
SLIGHTLY MOVABLE JOINTS
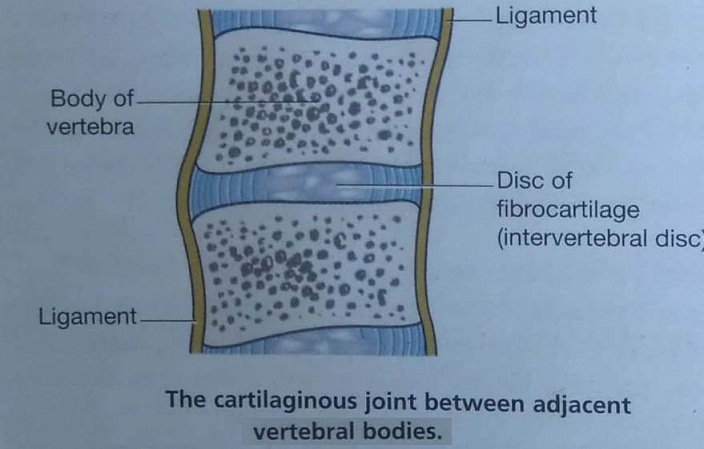
There
is a pad of fibro cartilage between the ends of the bones that form the joints
which allows for very slight movement where the p ad of cartilage is
compressed. Examples include the symphysis
pubis and the joints between the vertebral bodies.
3.
SYNOVIAL OR FREELY MOVABLE JOINTS
Synovial joints have characteristic features that enable a wide range of movement.

They
are classified according to the range of movement possible or to the shape of
the articulating parts of the bones involved.
·
Ball socket
·
Hinge joints
·
Gliding joints
·
Pivot joints
·
Condyloid
and saddle joints
A)
BALL AND SOCKET.

The head or ball of one bone
articulates with a socket of another and
the shape of the bones allows for a wide range of movement.
Those possible are flexion, extension,
adduction , abduction, rotation and circumduction. Examples are the shoulder and hip.
B)
HINGE JOINTS

These allows the movement of
flexion and extension only.
They are the elbow, knee , ankle , the joints
between the atlas and the occipital bone and the inter phalangeal joints of the
fingers and toes.
C)
GLIDING JOINTS

The articular surface
glide over each other example sternoclavicular
joints, acromioclavicular joints and joints between the carpal bones and
those between the tarsal bones.
D)
PIVOT JOINTS.

Movement is round one
axis example proximal and distal radioulnar joints and the joints between the
atlas and adontoid process of the axis.
E)
CONDYLOID AND SADDLE
JOINTS.

Movement takes
place round two axes, permitting flexion, extension, abduction, adduction and
circumduction example the wrist, temporo mandibular, metacarpophalangeal and
metatarsophlangeal joints.
HIT LIKE AND SHARE




























CHARACTERSTICS OF SYNOVIAL JOINT .

All synovial joints have certain characterstics in common.
1. Articular Or Hylaine Cartilage :
2. Capsule Or Capsular Ligament
3. Synovial Membrane
4. Other Intracapsular Structures
5. Extracapsular Structures
6. Nerve And Blood Supply .
v ARTICULAR OR HYLAINE CARTILAGE:

Ø The parts of the bones which are in contact are always covered with hyaline cartilage.
Ø It provides a smooth articular surface and is strong enough to absorb compression forces and bear the weight of the body.
Ø The cartilage lining , which is up to 7 mm thick in young people, becomes thinner and less compressible with age .
Ø This leads to increasing stress on other structures in the joint.
Ø Cartilage has no blood supply and receives its nourishment from synovial fluid.
v CAPSULE OR CAPSULAR LIGAMENT:

o The joint is surrounded and enclosed by a sleeve of fibrous tissue which holds the bones together.
o It is sufficiently loose to allow freedom of movement but strong enough to protect it from injury.
v SYNOVIAL MENBRANE :

This is composed of epithelial cells and is found.
1. Lining the capsule.
2. Covering those parts of the bones within the joint not covered by articular cartilage.
3. Covering all intracapsular structures that do not bear weight.
v SYNOVIAL FLUID :

· This is a thick sticky fluid, of egg-white consistency , secreted by synovial membranes into the synovial cavity.
· Little sacs of synovial fluid or bursae are present in some joints, e.g. the knee.
· They act as cushions to prevent friction between a bone and a ligament or tendon, or skin where a bone in a joint is near the surface.
FUNCTIONS:
1. Synovial fluid provides nutrients for the structures within the joint cavity .
2. Contains phagocytes , which remove microbes and cellular debris.
3. Act as a lubricant
4. Maintains joint stability
5. Prevents the ends of the bones from being separated , as does a little water between two glass surfaces.
v OTHER INTRACAPSULAR STRUCTURES:
· Some joints have structures within the capsule , but outside the synovial membrane ,which assist in maintenance of stability , e.g . fat pads and menisci in the knee joint.
· When these structures do not bear weight they are covered by synovial membrane.
v EXTRACAPSULAR STRUCTURES:
Ø LIGAMENTS that blend with the capsule provide additional stability at most joints.
Ø MUSCLES or their tendons also provide stability and stretch across the joints they move .
Ø When the muscle contracts it shortens , pulling one bone towards the other.
v NERVE AND BLOOD SUPPLY :
Nerves and blood vessels crossing a joint usually supply the capsule and the muscles that move it.
MOVEMENTS AT SYNOVIAL JOINTS.
movements at any given joint depends on various factors, such as the tightness of the ligaments holding the joint together ,how well the bones fit and the presence or absence of intracapsular structures.


HIP JOINT

v The ball and socket joint is formed b y the cup-shaped acetabulum of the innominate (hip) bone and the almost spherical head of the femur.
v The capsular ligament enclosed that head of the femur.
v The capsular ligament encloses the head and most of the neck of the femur.
v The cavity is deepened by the acetabular labrum, a ring of fibrocartilage attached to the rim of the acetabulum, with stabilizes the joint without liming its range of movement.
v The hip joint is necessarily a sturdy and powerful joint, since it bears all body weight when standing upright.
v It is stabilized by its surrounding musculature, but its ligaments are also important.
v The three main external ligaments are also important.
v The three main external ligaments are the iliofemoral, pubofemoral and ischiofemoral ligaments, which are localized thickenings of the joint capsule.
v Within the joint, the ligament of the head of the femur (ligamentum teres) attaches the femoral head to the acetabulum.
Muscles and movements.

The lower limb can be extended, flexed, abducted, adducted, rotated and circumducted at the hip joint.

KNEE JOINT
1. This is the largest and most complex joint.
2. It is a hinge joint formed by the condyles of the femur, the condyles of the tibia and the posterior surface of the patella.

3. The anterior part of the capsule is formed by the tendon of the quadriceps femoris muscle, which also supports the patella.
4. Intracapsular structures include two cruciate ligaments that cross each other, extending from the intercondylar notch of the femur to the intercondylar eminence of the tibia.
5. They help to stabilize the joint.
6. Semilunar cartilages or menisci are incomplete discs of white fibrocartilage lying on top of the articular condyles of the tibia.
7. They are wedge shaped, being thicker at their outer edges, and provide stability.
8. They prevent lateral displacement of the bones, and cushion the moving joint by shifting within the joint space according to the relative positions of the articulating bones.
9. Bursae and pads of fat are numerous.
10. They prevent friction between a bone and a ligament or tendon and between the skin and the patella. Synovial membrane covers the cruciate ligaments and the pads of fat.
11. The menisci are not convered with synovial membrane because they are weight bearing.
12. External ligaments of the joint provide further support, making it a hard joint to dislocate.
13. The main ligaments are the patellar ligament, an extension of the quadriceps tendon, the popliteal ligaments at the back of the knee and the collateral ligaments to each side.
Muscles and movements
v Possible movements at this joint are flexion, extension and a rotator movement that ‘locks’ the joint when it is fully extended.
v When the joint is locked, it is possible to stand upright for long periods of time without tiring the knee extensors.
v The main muscles extending the knee are the quadriceps femoris, and the principal flexors are the gastrocnemius and hamstrings.
WRIST JOINT
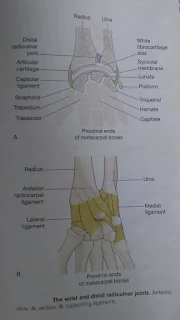















WRIST JOINT

v This is a condyloid joint between the distal end of the radius and the proximal ends of the scaphoid, lunate and triquetral.
v A disc of white fibrocartilage separates the ulna from the joint cavity and articulats with the carpal bones.
v It also separates the inferior radioulnar joint from the wrist joint.
v Extracapsular structures consist of medial and lateral ligament and anterior and posterior radiocarpal ligaments.
MUSCLES AND MOVEMENTS

1. The wrist can be flexed, extended, abducted and adducted.
2. The muscles that perform these movement are the main muscles that move the wrist.
JOINT OF THE HANDS AND FINGERS
1. There are synovial joints between the carpal bones, between the carpal and metacarpal bones, between the metacarpal bones and proximal phalanges and between the phalanges.

2. Movement at the hand and finger joints are controlled by muscles in the forearm and smaller muscles within the hand.
3. There are no muscles in the fingers; finger movements are produced by tendons extending from muscles in the forearm and the hand.
4. The joint at the base of the thumb is a saddle joint, unlike the corresponding joints of the other fingers, with are condyloid.
5. This means that the thumb is more mobile than the fingers and the thumb can be flexed, extended, circumducted, abducted and adducted.
6. In addition, the thumb can be moved across the palm to touch the tips of each of the fingers on the same hand (opposition), an ability that confers great manual dexterity and allows, for example, the holding of a pen and the fine manipulation of objects held in the hand.
7. The joints between the wrist and finger bones allow movement of the fingers.
8. The fingers may be flexed, extended, adducted, abducted and circumducted, with the first finger having the greatest flexibility of movement.
9. The finger joints are hinge joints, and allow only flexion and extension.
10. The flexor retinaculum is a strong fibrous band that stretches across the front of the carpal bones, enclosing their concavity and forming the carpal tunnel.
11. The tendons of flexor muscles of the wrist joint and the fingers and the medial nerve pass through the carpal tunnel, the retinaculum holding them close to the bones.
12. Synovial membrane forms sleeves around these tendons in the carpal tunnel and extends some way into the palm of the hand.
13. Synovial sheaths also enclose the tendons on the flexor surfaces of the fingers.
14. Their synovial fluid prevents friction that might damage the tendons as they move over the bones.
15. The extensor retinaculum is a strong fibrous band that extends across the back of the wrist.
16. Tendons of muscles that extend the wrist and finger joints are encased in synovial membrane under the retinaculum.
17. The synovial sheaths are less extensive than on the flexor aspect.
18. The synovial fluid secreted prevents friction.
ANKLE JOINT


ANKLE JOINT
The hinge joint is formed by the distal end of the tibia and its malleolus (medial malleolus), the distal end of the fibula (lateral malleolus) and the talus.

There are four important ligaments strengthening this joint: the deltoid and anterior, posterior, medial and lateral ligaments.
MUSCLES AND MOVEMENTS
The movements of inversion and eversion occur between the tarsal bones and not at the ankle joint. Ankle joint movements and the related muscles are shown in table

JOINTS OF THE FOOT AND TOES
There are a number of synovial joints between the tarsal bones, between the tarsal and metatarsal bones, between the metatarsals and proximal phalanges and between the phalanges.
Movements are produced by muscles in the leg with long tendons that cross the ankle joint, and by muscles of the foot.
The tendons crossing the ankle joint are encased in synovial sheaths and are held close to the bones by strong transverse ligaments. They move smoothly within their sheaths as the joints move. In addition to moving the joints of the foot, these muscles support the arches of the foot and help to maintain body balance.


SHOULDER JOINT

1. This ball and socket joint is the most mobile in the body, and consequently is the least stable and prone to dislocation, especially in children.
2. It is formed by the glenoid cavity of the scapula and the head of the humerus, and is well padded with protective bursae.
3. The capsular ligament is very loose inferiorly to allow for the free movement normally possible at this joint.
4. The glenoid cavity is deepened by a rim of fibrocartilage, the glenoidal labrum, which provides additional stability without limiting movement.
5. The tendon of the long head of the biceps muscle is held in the intertubercular (bicipital) groove of the humerus by the transverse humeral ligament.
6. It extends through the joint cavity and attaches to the upper rim of the glenoid cavity.
7. Synovial membrane forms a sleeve round the part of the tendon of the long head of the biceps muscles within the capsular ligament and covers the glenoidal labrum.
8. The joint is stabilized partly by a number of ligaments (the glenohumoral, coracohumeral and transverse humeral) but mainly by the muscles (and their tendons) present in the shoulder.
9. The stability of the joint may be reduced if these structures, together with the tendon of the biceps muscle, are stretched by repeated dislocations of the joint.
MUSCLES AND MOVEMENT.

The muscles that move the arm the muscles and movements possible at the shoulder joint.
ELBOW JOINT



ELBOW JOINT

1. This hinge joint is formed by the trochlea and the capitulum of the humerus, and the trochlear notch of the ulna and the head of the radius.

2. It is an extremely stable joint because the humeral and ulnar surfaces interlock, and the capsule is very strong.
3. Extracapsular structures consist of anterior, posterior, medial and lateral strengthening ligaments, which contribute to joint stability.
MUSCLES AND MOVEMENTS
Because of the structure of the elbow joint, the only two movements it allows are flexion and extension. The biceps is the main flexor of the forearm, aided by the brachialis; the triceps extends it.
PROXIMAL AND DISTAL RADIOULNAR JOINTS

1. The proximal radioulnar joint is a pivot joint formed by the rim of the head of the radius rotating in the radial notch of the ulna, and is in the same capsule as the elbow joint.
2. The annular ligament is a strong extracapsular ligament that encircles the head of the radius and keeps it in contact with the radial notch of the ulna.
3. The distal radioulnar joint is a pivot joint between the distal end of the radius and the head of the ulna.
4. Note, in addition, the presence of a fibrous membrane linking the bones along their shafts; this interosseous membrane is an example of the fibrous joint and prevents separation of the bones when force is applied at either end, i.e. at the wrist or elbow.
MUSCLES AND MOVEMENTS
The forearm may be pronated (turned palm down) or supinated (turned palm up). Pronation is caused by the action of the pronator teres and supination by the supinaotr and biceps muscles .
SKULL




SKULL

The skull rests on the upper end of the vertebral column and its bony structure is divided into two parts the cranium and the face.
CRANIUM




The cranium is formed by a number of flat and irregular bones that provide a bony protection for the brain .
It has a base upon which the brain rests and a vault that surrounds and covers it.
The periosteum inside the skull bones consists of the outer layer of dura mater.
The mature skull the joints (sutures) between the bones are immovable (fibrous).
The bones have numerous perforations (e.g.foramina,fissures) through which nerves,blood and lymph vessels.
The bones of the cranium are:


1 frontal bone
2 parietal bones
2 temporal bones
1 occipital bone
1 sphenoid bone
1 ethmoid bone .
FRONTAL BONE :

This is the bone of the forehead.
It forms part of the orbital cavities(eye sockets)and the prominent ridges above the eyes,the supra orbital margins.


Just above the supraorbital margins, within the bone, there are two air-filled cavities or sinuses lined with ciliated mucous membrane which have openings into the nasal cavity.
The coronal suture joins the frontal and parietal bones and other fibrous joints are formed with the sphenoid ,zygomatic ,lacrimal,nasal and ethmoid bones.
The bone orginates in two parts joined in the midline by the frontal suture.
PARIETAL BONES:

These bones form the sides of the roof of the skull.


Parietal bones articulate with each other at the sagittal suture, with the frontal bone at the coronal suture, with the occipital bone at the lamboidal suture and with the temporal bones at the squamous suture.
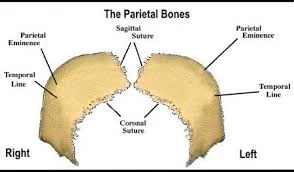

The inner surface is concave and is grooved by the brain and blood vessels.
TEMPORAL BONES:

These bones lie on each side of the head and form immovable joints with the parietal,occipital,sphenoid and zygomatic bones.
Each temporal bone has several important features.
The squamous part is the thin fan-shaped part that articulates with the parietal bone.
The zygomatic process articulates with the zygomatic arch(cheekbone).
The mastoid part contains the mastoid process, a thickened region behind the ear.
It contains a large number of very small air sinuses which communicate with the middle ear and are lined with squamous epithelium.
The petrous portion forms the part of the base of the skull and contains the organs of hearing(the spiral organ) and balance.
The temporal bone articulates with the mandible at the temporomandibular joint ,the only movable joint of the skull.
 munikrishnadn.blogspot.com
munikrishnadn.blogspot.com

FACE


The skeleton of the face is formed by 13 bones such as
2.zygomatic (cheek)bones
1 maxilla(originated as 2)
2 nasal bones
2 lacrimal bones
1 vomer
2 palatine bones
2 inferior conchae
1 mandible


Zygomatic (cheek) bones form the prominences of the cheeks and part of the floor and lateral walls of the orbital cavities.

This originates as two bones,but fusion takes place before birth.
The maxilla forms the upper jaw, the anterior part of the roof of the mouth,the lateral walls of the nasal cavity and part of the floor of the orbital cavities.


The alveolar ridge,or process, projects downwards and carries the upper teeth.
On each is a large air sinus,the maxillary sinus,lined with ciliated mucous membrane and with openings into the nasal cavity.
These are two small flat bones that form the greater part of the lateral and superior surfaces of the bridge of the nose.

These two small bones are posterior and lateral to the nasal bones and form part of the medial walls of the orbital cavities.


Each is pierced by a foramen for the passage of the nasolacrimal duct that carries the tears from the medial canthus of the eye to the nasal cavity.
The vomer is thin flat bone that extends upwards from the middle of the hard palate to form most of the interior part of the nasal septum.
Superiorly it articulates with the perpendicular plate of the etmoid bone.

These are two small L-shaped bones.


The horizontal parts unite to form the posterior part of the hard palate and the perpendicular parts project upwards to form part of the lateral walls of the nasal cavity.
At their upper extrimities they form part of the orbital cavities.

Each concha is a scroll-shaped bone, which forms part of the lateral wall of the nasal cavity and projects into it below the middle concha.


The superior and middle conchae are parts of the ethmoid bone.
The conchae collectively increase the surface area in the nasal cavity,allowing inspired air to be warmed and humidified more effectively.

This is the lower jaw , the only movable bone of the skull.
It originates as two parts that unite at the midline.


Each half consists of two main parts: a curved body with the alveolar ridge containing the lower teeth and a ramus,which projects upwards almost at right angles to the posterior end of the body.
At the upper end the ramus divides into the condylar process which articulates with the temporal bone to form the tempomandibular joint and the coronoid process, which gives attachement to muscles and ligaments that close the jaw.
The point where the ramus joins the body is the angle of the jaw.

This is an isolated horseshoe-shaped bone lying in the soft tissues of the neck just above the larynx and below the mandible.


It does not articulate with any other bone,but is attached to the styloid process of the temporal bone by ligaments.
It supports the larynx and gives attachment to the base of the tongue.
Immediately behind this articulating surface is the external auditory meatus (auditory canal),which passes inwards towards the petrous portion of the bone.


SPHENOID BONE :

Sphenoid bone occupies the middle portion of the base of the skull and it articulates with the occipital,temporal,parietal and frontal bones.
It links the cranial and facial bones ,and cross-braces the skull.

On the superior surface in the middle of the bone is a little saddle-shaped depression,the hypophyseal fossa (sella turcica) in which the pituitary glands rests.

The body of the bone contains some fairly large air sinuses lined with ciliated mucous membrane with openings into the nasal cavity.

OCCIPITAL BONE:

Occipital bone forms the back of the head and part of the base of the skull.
It has immovable fibrous joints with the parietal,temporal and sphenoid bones.


Its inner surface is deeply concave and the concavity is occupied by the occipital lobes of the cerebrum and by the cerebellum .
The occiput has two articular condyles that form condyloid joints with the first bone of the vertebral column,the atlas.


This joint permits nodding movements of the head. Between the condyles is the foramen magnum (meaning large hole) through which the spinal cord passes into the cranial cavity .
The first rib is firmly fixed to the sternum and to the first thoracic vertebra, and does not move during inspiration.
Because it is a fixed point, when the intercostals muscles contract, they pull the entire ribcage upwards towards the first rib.
follow us on: munikrishnadn.blogspot.com
VERTEBRAL COLUMN
















THORACIC CAGE


The thorax (thoracic cage) is formed by the sternum anteriorly, twelve pairs of ribs forming the lateral bony cages, and the twelve thoracic vertebrae.


STERNUM (BREAST BONE)
This flat bone can be felt just under the skin in the middle of the front of the chest.


The manubrium is the uppermost section and articulates with the clavicles at the sternoclavicular joints and with the first two pairs of ribs.
The body or middle portion gives attachment to the ribs.
The xiphoid process is the tip of the bone. It gives attachment to the diaphragm, muscles of the anterior abdominal wall and the linea alba.
RIBS.


The 12 pairs of ribs form the lateral walls of the thoracic cage.
They are elongated curved bones that articulate posteriorly with the vertebral column.
Anteriorly, the first 7 pairs of the ribs articulate directly with the sternum and are known as the true ribs.
The next 3 pairs articulate only indirectly. In both cases, costal cartilage attach the ribs to the sternum.
The lowest 2 pairs of ribs, referred to as floating ribs, do not join the sternum at all, their anterior tips being free.
They are elongated curved bones that articulate posteriorly with the vertebral column.
Anteriorly, the first 7 pairs of the ribs articulate directly with the sternum and are known as the true ribs.
The next 3 pairs articulate only indirectly. In both cases, costal cartilage attach the ribs to the sternum.
The lowest 2 pairs of ribs, referred to as floating ribs, do not join the sternum at all, their anterior tips being free.
Each rib forms up to three joints with the vertebral column.
Two of these joints are formed between facets on the head of the rib and facets on the bodies of two vertebrae, the one above the rib and the one below.
Ten of the ribs also form joints between the tubercle of the rib and the transverse process of (usually) the lower vertebra.
Two of these joints are formed between facets on the head of the rib and facets on the bodies of two vertebrae, the one above the rib and the one below.
Ten of the ribs also form joints between the tubercle of the rib and the transverse process of (usually) the lower vertebra.
The inferior surface of the rib is deeply grooved, providing a channel along which intercostals nerves and blood vessels run.
Between each rib and the one below are the intercostal muscles, essential for breathing.
Because of the arrangement of the ribs, and the quantity of cartilage present in the ribcage, it is flexible structure that can change its shape and size during breathing.Between each rib and the one below are the intercostal muscles, essential for breathing.
The first rib is firmly fixed to the sternum and to the first thoracic vertebra, and does not move during inspiration.
Because it is a fixed point, when the intercostals muscles contract, they pull the entire ribcage upwards towards the first rib.
follow us on: munikrishnadn.blogspot.com
VERTEBRAL COLUMN

Vertebral column is made by 26 bones.
24 separate vertebrae extend downwards from the occipital bone of the skull;then there is the sacrum,formed from five fused vertebrae,and lastly the coccyx,or tail,which is formed from between three to five small fused vertebrae, and lastly the coccyx, or tail, which is formed from between three to five small fused vertebrae.

The vertebral column is divided into different regions.
The first seven vertebrae, in the neck, form the cervical spine; the next twelve vertebrae are the thoracic spine and the next five the lumbar spine, the lowest vertebra of which articulates with the sacrum.
Each vertebra is identified by the first letter of its region in the spine, followed by a number indicating its position. For example, the topmost vertebra is called C1, and the third lumbar vertebra is called L3.
The movable vertebrae have many characteristics in common, but some groups have distinguishing features.
CHARACTERISTICS OF A TYPICAL VERTEBRA

THE BODY.
The body of each vertebra is situated anteriorly.
The size varies with the site.
They are smallest in the cervical region and become larger towards the lumbar region.
THE VERTEBRAL (NEURAL) ARCH.
This enclosed a large vertebral foramen.
It is the area behind the body, and forms the posterior and lateral walls of the vertebral foramen.
The lateral walls are formed from plates of bone called pedicles, and the posterior walls are formed from laminae.
Projecting from the regions where the pedicle meets the lamina is a lateral prominence called transverse process, and where the two laminae meet at the back is a process called the spinous process.
These are the bony prominences that can be felt through the skin along the length of the spine.
The neural arch has four articular surfaces; two articulate with the vertebra above the two with the one below.
The vertebral foramina form the vertebral (neural) canal that contains the spinal cord.
REGION-SPECIFIC VERTEBRAL CHARACTERISTICS
CERVICAL VERTEBRAE

These are the smallest vertebrae.

The transverse processes have a foramen through which a vertebral artery passes upwards to the brain.
The first two cervical vertebrae, the atlas and the axis, are typical.
The first cervical vertebra, the atlas, is the bone on which the skull rests.

Below the atlas is the axis, the second cervical vertebra (C2).
The atlas is essentially a ring of bone, with no distinct body or spinous process, although it has two short transverse processes.
It possesses two flattened facets that articulate with the occipigtal bone; these are condyloid joints and they permit nodding of the head.

The axis sits below the atlas, and has a small body with a small superior projection called the odontoid process (also called the dens, meaning tooth).
This occupied part of the posterior foramen of the atlas above, and is held securely within it by the transverse ligament.
The head pivots (i.e. turns from side to side) on this joint.
The seventh cervical vertebra C7, is also known as the vertebra prominens.
It possesses a long spinous prominence terminating in a swollen tubercle, which is easily felt at the base of the neck.
THORACIC VERTEBRAE.

The thoracic vertebrae are larger than the cervical vertebrae because this section of the vertebral column has to support more body weight.

The bodies and transverse process have facets for articulation with the ribs.
LUMBAR VERTEBRAE.

These are the largest of the vertebrae because they have to support the weight of the upper body. They have to support the weight of the upper body.
They have substantial spinous processes for muscle attachment.
SACRUM.

This consists of five rudimentary vertebrae fused to form a triangular or wedge-shaped bone with a concave anterior surface.
The upper part, or base, articulates with the 5th lumbar vertebra.
On each side it articulates with the ilium to form a sacroiliac joint, and at its inferior tip it articulates with the coccyx.
The anterior edge of the base, the promontory, protrudes into the pelvic cavity.
The vertebral foramina are present, and on each side of the bone there is a series or foramina for the passage of nerves.
COCCYX

This consists of the four terminal vertebrae fused to form a very small triangular bone, the broad base of which articulates with the tip of the sacrum.
FEATURES OF THE VERTEBRAL COLUMN
INTERVERTEBRAL DISCS

The bodies of adjacent vertebrae are separated by intervertebral discs, consisting of an outer rim of fibrocartilage (annulus fibrosus) and a central core of soft gelatinous material (nucleus pulposus). They are thinnest in the cervical region and become progressively thicker towards the lumbar region, as spinal loading increases.
The posterior longitudinal ligament in the vertebral canal helps to keep them in place.
They have a shock-absorbing function and the cartilaginous joints they form contribute to the flexibility of the vertebral column as a whole.
INTERVERTEBRAL FORAMINA.

When two adjacent vertebrae are viewed from the side, a foramen formed by a gap between the vertebral pedicles can be seen.
Half of the wall is formed by the vertebra above, and half by the one below.
Throughout the length of the column there is an intervetebral foramen on each side between every pair of vertebrae, through which the spine nerves, blood vessels and lymph vessels pass.
LIGAMENTS OF THE VERTEBRAL COLUMN.

These ligaments hold the vertebrae together and keep the intervertebral discs in position.
The transverse ligament maintains the odontoid process of the axis in the correct position in relation to the atlas.
The anterior longitudinal ligament extends the whole length of the column and lies in front of the vertebral bodies.
The posterior longitudinal ligament lies inside the vertebral canal and extends the whole length of the vertebral column in close contact with the posterior surface of the bodies of the bones.
The ligament flava connect the laminae of adjacent vertebrae.
The ligamentum nuchae and the supraspinous ligament connect the spinous processes, extending from the occiput to the sacrum.
CURVES OF THE VERTEBRAL COLUMN.

When viewed from the side, the vertebral column presents four curves: two primary and two secondary.
The fetus in the uterus lies curled up so that the head and the knees are more or less touching.
This position shows primary curvature.
The secondary cervical curve develops when the child can hold up his head (after about 3 months) and the secondary lumbar curve develops when he stands upright (after 12 to 15 months).
The thoracic and sacral primary curves are retained.
MOVEMENTS OF THE VERTEBRAL COLUMN
The movements between the individual bones of the vertebral column and very limited. However, the movements of the column as a whole are quite extensive and include flexion (bending forward), extension (bending backward), lateral flexion (bending to the side) and rotation. There is more movement in the cervical and lumbar regions than elsewhere.
FUNCTIONS OF THE VERTEBRAL COLUMN
These include the following:
· Collectively the vertebral foramina form the vertebral canal, which provides a strong bony protection for the delicate spinal cord lying within it.
· The pedicles of adjacent vertebrae form intervertebral foramina, one on each side, providing access to the spinal cord for spinal nerves, blood vessels and lymph vessels.
· The numerous individual bones enable a certain amount of movement.
· It supports the skull.
· The intervertebral discs act as shock absorbers, protecting the brain.
· It forms the axis of the trunk, giving attachment to the ribs, shoulder girdle and upper limbs, and the pelvic girdle and lower limbs.
SCAPULA

The scapula is a flat triangular-shaped bone.

The scapula is lying on the posterior chest wall superficial to the ribs and separated from them by muscles.

At the lateral angle is a shallow articular surface,the glenoid cavity ,which ,with the head of the humerus ,forms the shoulder joint .
On the posterior surface runs a rough ridge called SPINE, which extends beyond the lateral border of the scapula and overhangs the glenoid cavity.

The prominent overhanging , which can be felt through the skin as the highest point of the shoulder ,is called the ACROMION PROCESS and forms a joint with the clavicle , THE ACROMIOCLAVICULAR joint, a slightly movable synovial joint that contributes to the mobility of the shoulder gridle .
The CORONOID PROCESS , a projection from the upper border of the bone,gives attachment to muscles that move the shoulder joint.
Humerus

This is the bone of the upper arm.

The head sits within the glenoid cavity of the scapula ,forming the shoulder joint.
Distal to the head are two roughened projections of bone, the greater and lesser tubercular sulcus,occupied by one of the tendons of the biceps muscle.
The distal end of the bone presents two surfaces that articulate with the radius and ulna to form the elbow joint .
Ulna and radius .

These are the two bones of the forearm.

The ulna is longer than medial to the radius and when the arm is in the anatomical position, i.e. with the palm of the hand facing forward, the two bones are parallel.
They articulate with the humerus at the elbow joint, the carpal bones at the wrist joint and with each other at the proximal and distal radioulnar joints.

In addition , an interosseous membrane, a fibrous joint, connects the bones along their shafts, stabilizing their association and maintaining their relative positions despite forces applied from the elbow or wrist.
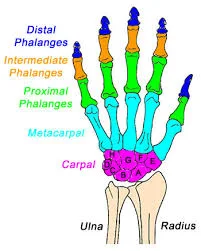

CARPAL BONES

There are eight carpal bones .
Carpal bones arranged in two rows
1. PROXIMAL ROW:scaphoid,lunate,triquetral,pisiform
2. DISTAL ROW: trapezium,trapezoid,capitates,hamate.

These bones are closely fitted together and held in position by ligaments that allow a limited amount of movement between them.
The bones of the proximal row are associated with the metacarpal bones.
Tendons of muscles lying in the forearm cross the wrist and are held close to the bones by strong fibrous brands,called RETINACULA.
METACARPAL BONES(BONES OF THE HAND)
Metacarpal are five bones form the palm of the hand.
They are numbered from the thumb side inwards.
The proximal ends articulate with the carpal bones and the distal ends with the phalanges.
PHALANGES(FINGER BONES)
There are 14 phalanges, three in each finger and two in the thumb.
They articulate with the metacarpal bones and with the metacarpal bones and with each other,by hinge joints.
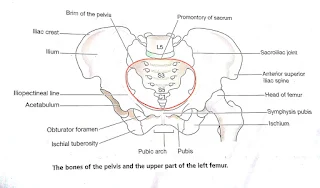
THE PELVIS

The pelvis is formed by the hip bones, the sacrum and the coccyx.
It is divided into upper and lower parts by the brim of the pelvis, consisting of the promontory of the sacrum and the iliopectineal lines of the innominate bones.

The greater or false pelvis is above the brim and the lesser or true pelvis is below.
DIFFERENCES BETWEEN MALE AND FEMALE PELVES:

The shape of the female pelvis allows for the passage of the baby during childbirth.
In comparison with the male pelvis, the female pelvis has lighter bones, is more shallow and rounded and is generally roomier.




THE PELVIC GIRDLE

The pelvic girdle is formed from two innominate (hip) bones.

The pelvis is the term given to the BASIN-SHAPED structure formed by the pelvic girdle and its associated sacrum.
INNOMINATE (HIP) BONES

Each hip bone consists of three fused bones: the ilium, ischium and pubis.
On its lateral surface is a deep depression, the acetabulum, which forms the hip joint with the almost-spherical head of femur.
The ilium is the upper flattened part of the bone and it presents the iliac crest, the anterior curve of which is called the anterior superior iliac spine.
The ilium forms a synovial joint with the sacrum, the sacroiliac joint, a strong joint capable of absorbing the stresses of weight bearing and which tends to become fibrosed in later life.

The pubis is the anterior part of the bone and it articulates with the pubis of the other hip bone at a cartilaginous joint, the symphysis pubis.
The ischium is the inferior and posterior part. The rough inferior projections of the Ischia, the ischial tuberosities, bear the weight of the body when seated.
The union of the three parts takes place in the acetabulum.


The femur is the longest and heaviest bone of the body.
The head is almost spherical and fits into the acetabulum of the hip bone to form the hip joint.

The neck extends outwards and slightly downwards from the head to the shaft and most of it is within the capsule of the hip joint.
The posterior surface of the lower third forms a flat triangular area called the popliteal surface.
The distal extremity has two articular condyles, which, with the tibia and patella, form the knee joint.
The function of the femur is to transmit the weight of the body through the bones below the knee to the foot.
TIBIA (SHIN BONE)

The tibia is the medial of the two bones of the lower leg.

The proximal extremity is broad and flat and presents two condyles for articulation with the femur at the knee joint.

The head of the fibula articulates with the inferior aspect of the lateral condyle, forming the proximal tibiofibular joint.
The distal extremity of the tibia forms the ankle joint with the talus and the fibula.
The medial malleolus is a downward projection of bone medial to the ankle joint.
FIBULA:

The fibula is the long slender lateral bone in the leg.
The head or upper extremity articulates with the lateral condyle of the tibia, forming the proximal tibiofibular joint, and the lower extremity articulates with the tibia, and projects beyond it to form the lateral malleolus.
This helps to stabilize the ankle joint.
PATELLA (KNEE CAP):

This is a roughly triangular-shaped sesamoid bone associated with the knee joint.

Its posterior surfaced articulates with the patellar surface of the femur in the knee joint and its anterior surface is in the patellar tendon, i.e. the tendon of the quadriceps femoris muscle.
TARSAL (ANKLE) BONES:

The seven tarsal bones forming the posterior part of the foot (ankle) are the talus, calcaneus, navicular, cuboid and three cuneiform bones.

The talus articulates with the tibia and fibula at the ankle joint.
The calcaneus forms the heel of the foot.
The other bones articulate with each other and with the metatarsal bones.
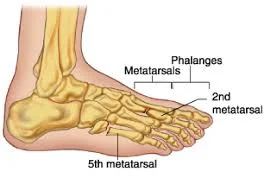
METATARSALS (BONES OF THE FOOT):

There are five bones, numbered form inside out, which form the greater part of the dorsum of the foot.

At their proximal ends they articulate with the tarsal bones and at their distal ends, with the phalanges.

The enlarged distal head of the 1st metatarsal bone forms the ‘ball’ of the foot.
PHALANGES (TOE BONES):

There are 14 phalanges arranged in a similar manner to those in the fingers, i.e. two in the great toe (the halux) and three in each of the other toes.

ARCHES OF THE FOOT.

The arrangement of bones in the foot, supported b y associated ligaments and action of associated muscles, gives the sole of the foot an arched or curved shape.
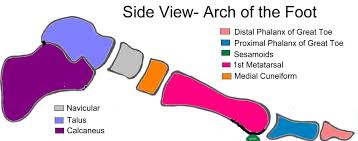
The curve running from heel to toe is called longitudinal arch, and the curve running across the foot is called the transverse arch.
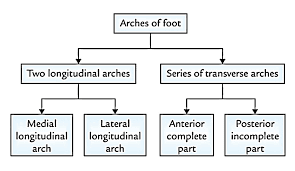
In the normal longitudinal arch, only the calcaneus and the distal ends of the metatarsals should touch the ground, the bones in between lifted clear.
This gives a conventional footprint shape.
If, however, the concavity of the sole is lost because of sagging ligaments or tendons, the arch sinks and much more of the sole of the foot is in contact with the ground; this is called flat foot.
Because the arches of the foot are important in distributing the weight of the body evenly whilst upright, whether stationary or moving, the flat foot loses the springiness of normal foot structure and leads to sore feet when standing, walking or running for long periods.
As there are movable joints between all the bones of the foot, very strong muscles and ligaments are necessary to maintain the strength, resilience and stability of the foot during walking, running and jumping.
POSTERIOR TIBIALIS MUSCLE.
This is the most important muscle support of the longitudinal arch.
It lies on the posterior aspect of the lower leg, originates from the middle third of the tibia and fibula and its tendon passes behind the medial malleolus to be inserted into the navicular, cuneiform, cuboid and metatarsal bones. It acts as a sling or ‘suspension apparatus’ for the arch.
SHORT MUSCLES OF THE FOOT.
This group of muscles is mainly concerned with the maintenance of the longitudinal and transverse arches. They make up the fleshy part of the sole of the foot.
PLANTAR CALCANEONAVICULAR LIGAMENT (‘SPRING’ LIGAMENT).
This is very strong thick ligament stretching from the calcaneus to the navicular bone. It plays an important part in supporting the medial longitudinal arch.
Plantar ligaments and interosseous membranes. These structures support the lateral and transverse arches.
Fractures are classified into different categories.








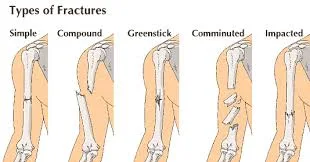
FRACTURES
When a bone breaks it is termed as a fracture.
Types of fractures

Fractures are classified into different categories.
1. SIMPLE OR CLOSED FRACTURE :

bone breaks in one place and no serious damage is done to the surrounding tissues .
2. COMPLICATED FRACTURE :

bone is broken and the break causes injury of the surrounding soft tissues.
3. COMPOUND OR OPEN FRACTURE :

Bone is broken and one or both ends protrude through the skin.
4. COMMINUTED FRACTURE :

it is one where the bones broken at a number of places.

5. IMPACTED FRACTURE :

it is one where the bone is broken and one end is driven into the other.
6. GREENSTICK FRACTURE :

here only one side of the shaft is broken, and the other is bent. This usually occurs in children whose long bones have yet to fully ossify.
7. SPIRAL FRACTURE :

it is produced by twisting stresses,spread along the length of the bone.
8. COLLE’S FRACTURE :

it is a break in the distal portion of the radius . it is often the result of reaching out to cushion a fall.

%20d%20trans.jpg)





{kind=link}
0 Comments