SPINAL
DISC HERNIATION:
 |
| Spinal Disc Herniation |
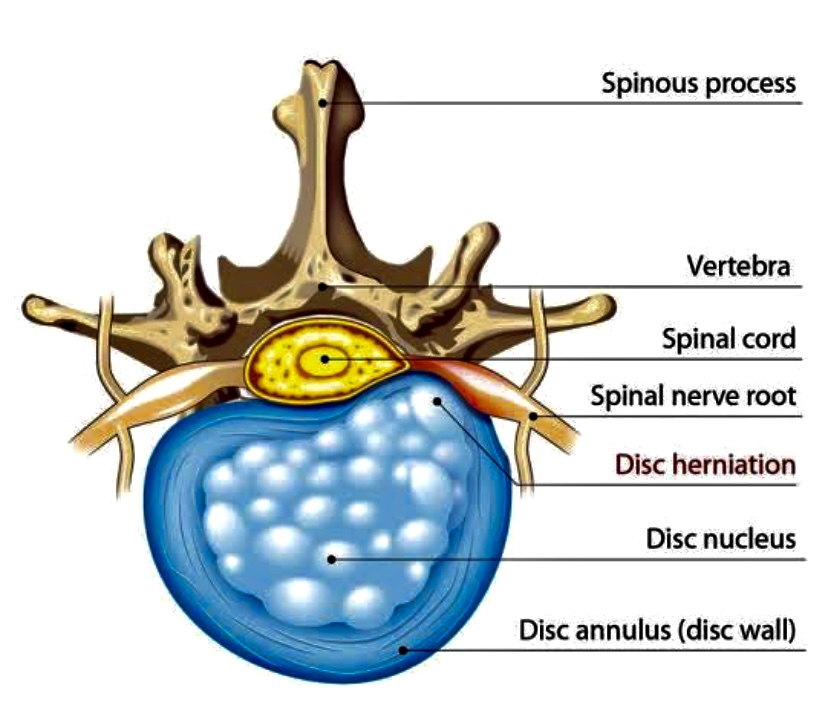
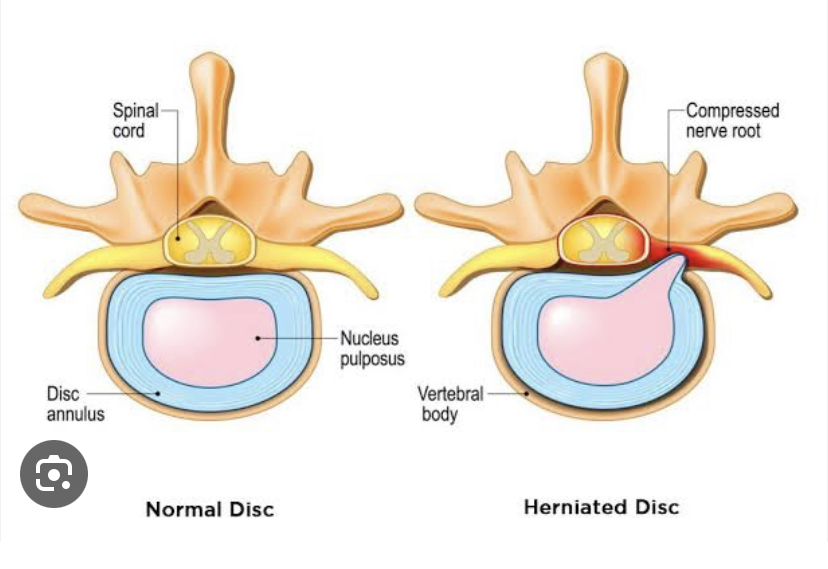
A spinal disc herniation informally
and misleadingly called a “slipped disc”
is a medical condition affecting the spine, in which a tear in the outer,
fibrous of an intervertebral disc allows the soft, central portion to bulge
out.
Stages
of Spinal Disc Herniation:
M
Disc herniation can occur in any disc in
the spine, but the two most common form are lumbar disc herniation. The former
is the most common, causing lower back pain and often leg pain as well, in
which case it is commonly referred to as sciatica.
Cervical disc herniations occurs in the neck, most often between the fifth
& sixth (C5/6) and the sixth and seventh (C6/7) cervical vertebral bodies.
Symptoms can affect the back of the skull, the neck, shoulder girdle, scapula,
shoulder, arm, and hand. The nerves of the cervical plexus and brachial plexus
can be affected.
Thoracic
disc herniation:
Thoracic discs are very stable and
herniations is this region are quite rare. Herniation of the uppermost thoracic
disc can mimic cervical disc herniations, while herniation of the other discs
can mimic lumbar herniations.
Lumbar
disc herniation:
Lumbar disc herniations occurs in the
lower back, often between the fourth and fifth lumber vertebral bodies or
between the fifth and the sacrum.
MRI
scan of large herniation (on the right) of the disc between the L4-L5
vertebrae.
Cervical
Disc Herniation:
·
Pain
& Muscle Spasm in neck.
·
Decreased
range of motion secondary to pain.
·
Unilateral
hand and arm pain.
·
Numbness
& tingling (paresthesia) in upper extremities.
·
Weakness
of upper extremity.
Lumbar
Disc Herniation:
·
Low
back pain with sensory and motor dysfunction.
·
Pain
radiating from lower back into the buttocks and down the leg.
·
Paresthesia,
weakness and reflex impairment.
·
Muscle
spasm.
·
Decreased
range of motion.
DIAGNOSIS:
1) Neurological Examination:
Straight
leg raise:
The straight leg raise may be
positive, this finding has low specificity; however it has high sensitivity.
Imaging
·
X-ray
studies
·
Computed
tomography scan (CT or CAT scan)
·
Magnetic
resonance Imaging (MRI)
2)
Myelogram: An x-ray of the
spinal canal following injection of a contrast material into the surrounding
cerebrospinal fluid spaces. By revealing displacement of the contrast material,
it can show the presence of structures that can cause pressure on the spinal
cord or nerves, such as herniated discs, tumors, or bone spurs.
3)
Electromyogram
and Nerve conduction studies (EMG/NCS): These tests measure the electrical impulse
along nerve roots, peripheral nerves, and muscle tissue. This will indicate
whether where is ongoing nerve damage, if the nerves are in a state of healing
from a past injury, or whether there is another site of nerve compression.
MANAGEMENT:
The majority of herniated discs will
heal themselves in about six weeks and do not require surgery. One study found
that ``After 12 weeks, 73% of patient showed reasonable to major improvement
without surgery.``
Pain medication are often prescribed
to alleviate the acute pain and allow the patient to begin exercising and
stretching.
There are a variety on non-surgical
alternatives used in treatment of the condition, which may or may not help:
1)
Rest
and activity modification- Complete rest and avoidance of activities that
aggravate symptom are recommended.
2)
Physical
therapy
3)
Massage
therapy
4)
Ice
& heat applications
5)
Non-steroidal
anti-inflammatory drugs (NSAIDs) e.g, Zerodol.
6)
Oral
steroids (e.g. prednisone or methylprednisolone)
7)
Epidural
(cortisone) injection
8)
Intravenous
sedation, analgesia-assisted traction therapy (IVSAAT)
9)
Weight
control
SURGERY:
Surgery should only be considered
as a last resort after all conservative treatments (non-surgical therapy) have
been tried, that did not alleviate the pain and heal the disc herniation.
Surgery is indicated if a patient
has a significant neurological deficit. The presence of cauda equina syndrome
(in which there is incontinence, weakness and genital numbness) is considered a
medical emergency requiring immediate attention and possibly surgical decompression.
Surgical options include:
Surgical goals include relief or nerve
compression, allowing the nerve to recover, as well as the relief of associated
back pain and restoration of normal function.
·
Chemonucleolysis
– dissolves the protruding disc
·
IDET
(a minimally invasive surgery for disc pain)
·
Discectomy/Microdiscectomy
– to relieve nerve compression
·
Laminectomy
– to relieve spinal stenosis or nerve compression
·
Hemilaminectomy
– to relieve spinal stenosis or nerve compression
·
Lumbar
fusion (lumbar fusion is only indicated for recurrent lumbar disc herniations,
not primary herniations)
·
Anterior
cervical discectomy and fusion (for cervical disc herniation)
·
Disc
arthroplasty (experimental for cases of cervical disc herniation)
·
Dynamic
stabilization
·
Artificial
disc replacement, a relatively new form of surgery in the U.S. but has been in
use in Europe for decades, primarily
used to treat low back pain from a degenerated disc.
·
Nucleoplasty
NURSING
MANAGEMENT OF PATIENT WITH A CERVICAL DISCECTOMY:
Nursing
diagnosis:
1. Pain related to
the surgical procedure.
2. Impaired
physical mobility related postoperative surgical regimen.
3. Knowledge
deficit about the postoperative course and home care management.
Nursing
Interventions:
1) Relieving Pain:
·
The
patient may be kept flat in bed for 12 to 24
·
Monitoring
the donor site for hematoma formation
·
Administering
the prescribed postoperative analgesic,positioning for comfort
·
Reassuring
the patient that the pain can be relieved
·
A
pure diet may be given if the patient has dysphagia
·
2) Improving Mobility:
·
Assess
the mobility of patient
·
A
cervical collar is usually worn, which contributes to limited neck motion and
altered mobility
·
Patients
are instructed to turn the body instead of the neck when looking from side to
side
·
Patient
are assisted during position changes, making sure that head, shoulder and
thorax are kept aligned.
3) Teaching patients self care:
·
A
cervical collar is usually worn for about 6 weeks
·
The
patients are instructed in care and use of the cervical collar
·
Patients
are instructed to alternate tasks in which the body does not move
·
The
patient is instructed about strategies for pain management.







{kind=link}
0 Comments