RESPIRATION
RESPIRATION:-
“The term respiration means the exchange of gases between body cells & the environment. this involves two main process:
1. Breathing [Pulmonary ventilation]
This is movement of air into and out of the lungs.
2. Exchange of Gases:-
It takes place
· In the lungs- external respiration.
· In the Tissues- Internal respiration.
Breathing:-
Breathing supplies O2 to the alveoli & Eliminates Co2.
MUSCLES OF BREATHING:-
Expansion of the chest during inspiration occurs as a result of muscular activity, partly voluntary & partly involuntary.
The Main Muscles of Breathing are:
1. Intercostal Muscles
2. Diaphragum.
INTERCOSTAL MUSCLES:-
1. There are 11 pairs of intercostals muscles that occupy the space between the 12 pairs of ribs.
2. They are arranged in two layers, the external & Internal muscles.
THE EXTERNAL INTERCOSTALS MUSCLE FIBRES:-
These exted downwards & forwards from the lower border of the rib above to the upper border of the rib below.
THE INTERNAL INTERCOSTALS MUSCLE FIBRES:-
1. These extend downwords & forwards from the lower border of the rib below, crossing the external intercostals muscle fibres at rt angels.
2. The first rib is fixed, therefore, when the intercostals muscle contract they pull all the other ribs downwords the first rib.
3. The shape & sizes of the ribs they move outwords when pulled upwords, enlarging the thoracic covity.
4. The intercostals muscles are stimulated to contract by the intercostals nerves.
DIAPHRAGM
1. The diaphragm is a dome-shaped muscular structure separating the thoracic & abdominal cavities.
2. It forms the floor of the thoracic cavity & the roof of the abdominal cavity & consists of a central tendor from which muscle fibres radiate to be attached to the lower ribs & sternum & to the vertebral column by two crura.
3. When the muscle of the diaphragm is relaxed the central tendor is at the level of 8th theoracic Vertebra.”
4. When it contract its muscle fibres shorten & the central tender is pulled downwords to the level of the 9th thoracic Vertebra, enlarging the thoracic cavity in length.
5. This decreases pressure in the thoracicavity & increases it in the abnormal & pelvic cavities.
6. The diphragm is supplies by the “Phrenic nerves”
7. The intercostals muscles & the diaphragm contract simmulatenously enlarging the thoracic cavity in tall direction that it from back to front, side to side & top to top.
CYCLE OF BREATHING
The average respiratory rate is 12 to 15 breaths per minute
Each breath consists of there phases.
1. Inspiration
2. Expiration
3. Pause.
LARYNX





These processes continue as inspired air travels through the larynx.
Trachea


LUNGS.





BRONCHI & BRONCHIOLES

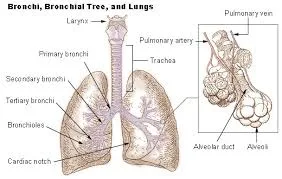
ALVEOLI



LARYNX
1.INTRODUCTION:
Larynx is also called it has “voicebox” ,which extends from the root of the tongue and hyoid bone to the trachea.
2.SITUATION:
It lies infront of the laryngopharynx at the level of 3rd ,4th ,5th and the 6th cervical vertebrae.
3.SHAPE:
APPLE SHAPE
APPLE SHAPE
Upto the puberty there is little difference between two sexes ,there after it grows larger in male compare to females,which explains prominence of the “adam`s apple ” and it gives deeper voice.
4.STRUCTURES ASSOSCIATED WITH THE LARYNX.
§ Superiorly – The Hyoid Bone And The Root Of The Tongue.
§ INFERIORLY – It Is Continous With The Trachea.
§ ANTERIORLY-The Muscles Attached To The Hyoid Bone And The Muscles Of The Neck.
§ POSTERIORLY- The Laryngophaynx And 3rd To 6th Cervical Vertebrae.
§ Laterally- The Lobes Of The Thyroid Gland.
5.structure:

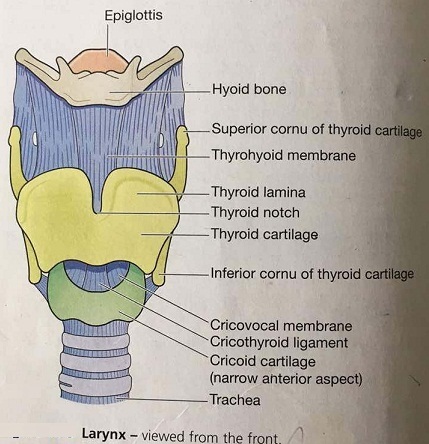
CARTILAGES:
The larynx is composed of many irregularly shaped cartilages attatched to each other by ligaments and membranes.
They are
Hyaline cartilage
v 1 thyroid cartilage
v 1 cricoid cartilage.
v 2 arytonoid cartilages
Elastic fibrocartilage
v 1 epiglottis.
The thyroid cartilage:
v This is the most prominent & consists of two flat pieces of hyaline cartilage or laminae,fused anteriorly , forming the laryngeal prominence( ADAM`S APPLE).
v Immediately above the laryngeal prominence the laminae are separated ,forming a V shaped notch called it has THYROID NOTCH.
v In posterior region the thyroid cartilage is incomplete and the posterior border of each lamina is extended to to form 2 process called the SUPERIOR and INFERIOR CORNU.
v The upper part of the thyroid cartilage is lined with stratified squamous epithelium .
v The lower part lined with ciliated columnar epithelium like the trachea.
v The thyroid cartilage forms most of the anterior and lateral walls of the larynx.
THE CRICOID CARTILAGE:

Ø This lies below the thyroid cartilage and composed with hyaline cartilage.
Ø It is signet ring shaped completely encircling the larynx with the narrow part anteriorly and the broad part posteriorly.
Ø It also lined with ciliated columnar epithelium with muscles and ligaments attaches to its outer surface.
Ø The lower border of the cricoids cartilage marks the end of the respiratory tract.
THE EPIGLOTTIS.
1.It is a LEAF shaped fibrocartilage attachéd to the inner surface of the anterior wall of the thyroid cartilage.
2. it is covered with strartified squamous epithelium.
3. if the larynx is likened to a box then the epiglottis is acts as the lid, it closes off the larynx during swallowing , protecting the lungs from accidental inhalation of foreign substances.
THE ADENOID CARTILAGES.
Ø These are two roughly pyramid – shape hyaline cartilage.
Ø It Suitated On Top Of The Broad Part Of The Cricoids Cartilage Forming Part Of The Posterior Wall Of The Larynx.
LIGAMENTS AND MEMBRANES
There are several ligaments that attaches the cartilages to each other end and to the hyoid bone.
6.BLOOD SUPPLY
ARTERIAL SUPPLY:Superior and inferior laryngeal arteries.
VENOUS DRAINAGE: The thyroid veins , which joins the internal jugular vein .
7. NERVE SUPPLY:
PARASYMPATHETIC NERVE SUPPLY:
From the superior laryngeal nerves which are branches from the VAGUS nerve.
SYMPATHETIC NERVE SUPPLY:
From the superior cervical ganglia , one on each side.
8.INFERIOR OF THE LARYNX.

The vocal cords are two pale folds of mucus membrane with cord-like free edges.

The space between the vocal cords is called GLOTTIS.
9.FUNCTIONS
1. PRODUCTION OF SOUND
Sound has the properties of pitch,volume and resonance.
2. SPEECH:
This occurs during expiration when the sounds produced by the vocal cords are manipulated by the tongue,cheeks and lips.
3. Protection of the lower respiratory tract.
1. While swallowing of the food the larynx moves upwards, occluding opening it from the pharynx and the hinged epigilttis closes over the larynx.
2. This Ensures That Food Passes Into The Oesophagus And Not Into The Lower Respiratory Passages.
4.PASSAGE FOR AIR.
This is between the pharynx and trachea.
5.Humidifying, filtering and warming.
These processes continue as inspired air travels through the larynx.
Trachea
1. Introduction:
The trachea is also called it as “WINDPIPE”.
2. Situation:
It is situated at the level of 5th thoracic vertebra where it divides at the carina into the right and left primary bronchi, one bronchous going to each lung.
3. Measurments:
v Length : approximately 10-11cm long
v SHAPE: WIND PIPE.
4. Structures associated with the trachea
v SUPERIORLY: the larynx
v INFERIORLY: the right and left bronchi
v Anteriorly: Upper part: the isthmus of the thyroid gland .
§ Lower part: the arch of the aorta and the sternum.
v POSTERIORLY: The oesophagus separates the trachea from the vertebral column.
v Laterally : The lungs and the lobes of the thyroid gland.
5. Structure :

v Trachea is composed of 3 layers of tissue (C-shape) rings of hyaline cartilage lying one above another.
v The rings are incomplete posteriorly.
v Connective tissue and involuntary muscle join the cartilages and form the posterior wall where the rings are incomplete.
v The soft tissue posterior wall is in contact with the oesophagus .
Three layers of tissue “CLOTHE” the cartilages of the trachea.
1. The outer layer consists of fibrous and elastic tissue and encloses the cartilages.
2. The middle layer consists og cartilages and bands of smooth muscle that wind round the trachea in a helical arrangement.
3. The inner lining consists of ciliated columnar epithelium, containing mucus-secreting goblet cells.
6. Blood supply
v Arterial Supply : The inferior thyroid and bronchial arteries.
v Venous drainage: Inferior thyroid veins into the brachiocephalic veins.
7. Nerve supply
Para sympathetic nerve supply :
v The recurrent laryngeal nerves and other branches of the vagi.
v Para sympathetic stimulation constricts the trachea.
Sympathetic nerve supply:
v Nerve supply from the sympathetic ganglia.
v Sympathetic stimulation dilates the trachea.
8. Lymphatic supply:
v Lymph from the respiratory passages drains through lymph nodes situated round the trachea and in the carina.
v The area where it divides into two bronchi.
9. Functions
1. SUPPORT AND PATENCY :
v The arrangement of cartilage and elastic tissue prevents kinking and obstruction of the airways as the head and neck move.
2. MUCOCILIARY ESCALATOR:

v This is the synchronous and regular beating of the cilia of the mucous membrane lining that wafts mucus with adherent particles upwards towards the larynx, where it is either swallowed or coughed up.
3. COUGH REFLEX.
v Nerve endings in the larynx, trachea and bronchi are sensitive to irritation, which generates nerve impulses conducted by the vagus nerves to the respiratory centre in the brain stem.
4. WARMING, HUMIDIFYING AND FILTERING.
v These continue as in the nose, although air is normally saturated and at body temperature when it reaches the trachea.
10. Applied anatomy:
TRACHEITIS: Inflammation of the trachea.
v The infection may occur especially in tobacco smokers and people who live or work in a polluted atmosphere.
LUNGS.
1.INTRODUCTION:

These are pair of airfilled structure in the respiratory system.
2.SITUATION :
Two lungs lying on each side of the midline in the thoracic cavity.
3.MEASURMENTS
SHAPE: CONE
REGIONS :
APEX
BASE
COSTAL SURFACE
MEDIAL SURFACE
4.ORGANS ASSOSCIATED WITH LUNGS:

APEX:
v It is rounded and rises into the root of the neck.
v About 25 mm above the level of the middle third of the clavicle
v It lies close to the first rib and blood vessels and nerves in the root of the neck.
THE BASE:
v This is concave and semilunar in shape.
v Lies on the thoracic surface of the diaphragm.
THE COSTAL SURFACE:
v This surface is convex in shape.
v Lies against the costal cartilages, the ribs and the intercostals muscles.
THE MEDIAL SURFACE:
v This surface is concave and roughly triangular-shaped area called “HILUM”.
v It lies at the level of the 5th,6th and 7th thoracic vertebrae.
v Structures forming the root of the lung enter and leave at the hilum.
v The area between the lungs is called “MEDIASTINUM”.
v It is occupied by the heart,greatvessels,trachea,right and left bronchi,oesophagus,lymph nodes,lymph vessels and nerves.
v The right lung is divided into three distinct lobes
· SUPERIOR LOBE
· MIDDLE LOBE
· INFERIOR LOBE
v The left lung is smaller because the heart occupies space left of the midline.
v It is divided into two lobes
SUPERIOR And INFERIOR LOBE.
5.GROSS STRUCTURE :

PLEURA AND PLEURAL CAVITY:

v The pleura consists of a closed sac of serous membrane(one for each lung) which contains a small amount of serous fluid.
v The lung is invaginated (pushed into) this sac so that it forms two layers: one adhers to the lung and the other to the wall of the thoracic cavity.
v THE VISCERAL PLEURA: This is adherent to the lung, covering each lobe and passing into the fissures that separate them.
v THE PARIETAL PLEURA: This is adherent to the inside of the chest wall and the thoracic surface of the diaphragm.
v It remains detached from the adjacent structures in the mediastinum and continous with the visceral pleura round the edges of the hilum.
v THE PLEURAL CAVITY: This is only a potential space.
v The two layers of pleura are separated by a thin film of serous fluid which allows them to glide over each other.
v It prevents friction between them during breathing.
v The serous fluid is secreted by the epithelial cells of the membrane.
The two layers of pleura, with serous fluid between,behave in the same way as two pieces of glass separated by a thin film of water.
They glide over each other easily but can be pulled apart only with difficulty,because of the surface tension between the membranes and the fluid.
If either layer of pleura is punctured,the underlying lung collapses owing to its inherent property of elastic recoil.
INFERIOR OF THE LUNGS:
The lungs are composed of the bronchi and smaller air passages,alveoli, connective tissue,blood vessels,lymphvessels and nerves, all embeddednin an elastic connective tissue matrix.
6.BLOOD SUPPLY:

ARTERIAL SUPPLY :
The pulmonary trunk divides into the right and left pulmonary arteries,it carries pure blood .
VENOUS DRIANAGE :
two pulmonary bronchial veins carry the de-oxygenated blood.
7.NERVE SUPPLY:
PARASYMPATHETIC NERVE SUPPLY:
The vagus nerves stimulate contraction of smooth muscle in the bronchial tree causing BRONCHOCONSTRUCTION.
SYMPATHETIC NERVE SUPPLY:
Stimulation causes BRONCHODILATATION.
Stimulation causes BRONCHODILATATION.
8.LYMPHATIC SUPPLY :
Lymph is drained from the walls of the air passages in a network of lymph vessels.
It passes through lymph nodes situated around the trachea and bronchial tree then into the thoracic duct on the left side and right lymphtic duct on the other.
9.FUNCTIONS:
Control of air entry.
Warming and humidifying
Support and patency.
Cough reflex.
BRONCHI & BRONCHIOLES

1. INTRODUCTION:- “ A Bronchus also brown as a main (or) primary bronchus, is an airway in the respiratory tract that conducts air into the lungs.
2. SITUATION: - The Level of the 5th thoracic Vertebra
3. PARTS:-


The Right Bronchus.
The Left Bronchus.
RT BRONCHUS:-




1. This is wider, shorter & more vertical than the lt bronchus & is therefore more likely to become obstructed by an inhaled foreign body.,
2. Length:- Approximately-2.5 cm long.
3. After entering the Rt lung at the hilum it divides into three branches Out to each lobe.
LT BRONCHUS:-
1. This is about 5cm long & is narrow than the right.
2. After entering the lung at the hilum it divides into two branches, one to each lobe ,
3. Each branch then sub divides into progressively smaller tubes within the lung Substance.
4. STRUCTURE:-.

· The bronchi are composed of the same tissues as the Trachea, and are lined with ciliated columnar epithelium.
· The bronchi subdivided into branchioles, terminal bronchioles, respiratory bronchioles, alveolar ducts & aveoli.
· The distal end of the bronchi the cartilages become irregular in shape and are absent at bronchiolar level.
· In the absence of cartiliage the smooth muscle in the walls of the bronchioles became thicker & is responsive to autonomic nerve stimulation & irritation.
· Ciliated coloumnar mucus memberane changes gradually to non-ciliated cuboidal-shaped calls In the distal bronchioles.
· The wider passage are called conducting airways.
· Conducting airways function is to bring air into the lungs & their walks are too thick to permit gas exchange.
5. BLOOD SUPPLY:-
Arterial Supply :- the Rt & Lt Bronchial arteries.
Venous Returns:- Bronchial veins.
6. NEVER SUPPLY:- Parasympathetic:- Vagus nerve Stimulates contraction of smooth muscle causes “ Branchoconstriction.
Sympathetic nerve supply: Stimulation causes Bronchodilation.
7. LYMPH SUPPLY:- Lymph is drained from the walls of the air passages in a network of lymph vessels.

1. INTRODUCTION:- the tiny air sacs of the lungs which allow for rapid gaseous exchange of O2 & Co2.
2. SITUATION:- Inside of the lungs & ovules.
3. STRUCTURE:-

1.The Lung Issue is further divided by time shets of connective tissue into lobules.
2. Each labule is supplied with air by a terminal bronchiole, which further subdivides into respiratory brancioles, a aleveloar ducts & lorge no of alveols.
3. there are more than 150 million alveli in the adult lung.
4. As Airways divides & become smaller & Smaller their walks gradually become thinner until muscle and connective tissue disappear,leaving a single layer of simple squammous epithelial cells in the alveolar ducts & alveoli.
5. The Alveoli are surrounded by a dense network of capillaries.

6. Exchange of gases in the lung (external respiration) takes place across a memberane made up of the alveolar wall & the capillary wall fused firmly together this process called “ Respiratory membrance”
7. Lying between the squamous cells are septal cells that secrate surfactant ,a phospolipid fluid which prevents the alveoli from drying out.
8. Surfactant Reduces surface tension & preve alveolar walls collapsing during expiration.
9. secretion of surfactant into the distal air passage & alveoli begins about the 35th week of fetal life.
10. improper function of alveoli in the premature babies causes serious breathing problems.
NERVE SUPPLY:
PARASYMPATHETIC:- The Vagus nerve causes bronchocostriction.
SYMPATHETIC NS :- Stimulation relaxes brounchiolar smooth muscle.

%20d%20trans.jpg)






{kind=link}
0 Comments