HEART

1. INTRODUCTION:
The heart is the roughly hollow muscular organ.
2. SITUATION:

Ø The heart lies in the thoracic cavity in the mediastinum between the lungs.
Ø It lies obliquely a little more to the left than the right and presents a base above & an apex below.
3. MEASURMENTS:
Ø SHAPE - CONE SHAPE
Ø LENGTH - 10 cm long
Ø SIZE - 225 gm in women.
More than 225 gm in Men.
4. ORGANS ASSOCIATED WITH THE HEART:

Ø Inferiorly – the apex rests on the central trends of the diaphragm.
Ø Superiorly- Blood venal that is the aorta, SVC, Pulmonary artery & Pulmonary veins.
Ø Posteriorly - The Oesophagus, trachea, left & right bronchus, m Descending aorta, IVC & thoracic vertebrae.
Ø Laterally - The lungs the left lung overlaps the left side of the heart.
Ø Anterior - The sterum, Ribs & Intercostal muscles.
5. STRUCTURE:

The heart is composed of 3 layers
Ø Pericardium
Ø Myocardium
Ø Endocardium
PERICARDIUM:
It is the outer conversing layer of the heart, made up of 2 sacs.
Ø Other sac - commits fibrous tissue
Ø Inner sac - Double layer of Serous membrane.
The outer fibrous sac is continuous. With the tunica adventitia of the great blood vessels above and is adherent to the diaphragm below.
Ø It’s in elastics, fibrous nature.
Ø The outer layer of the serous membrane, the parietal pericardium, lines the fibrous sac.
Ø The Inner layer, the visceral pericardium or epicardium, which is continuous with the parietal pericardium, is adherents to the heart muscle.
Ø Serous membrane consists of flattened epithelial cells.
Ø It secretes serous third into the space between the visceral & parietal layers which allows smooth movement between them when the heart beats.
Ø The between the parietal & visceral pericardium is only a potential space.
MYOCARDIUM:

The Myocardium is composed of specialized cardiac muscle found only in the heart.
Ø It is not under voluntary control but like skeletal muscle, cross stripes are seen on microscopic examinations.
Ø Each fibre has nuclei and one or more branches.
Ø Microscopically these Joints or Intercalated discs can be seen as thicker,darker lines than the ordinary cross stripes.
Ø When an impulse is initiated. It spreads from cell to cell via the branches and intercalated discs over the whole sheet of muscle, causing contraction.
Ø The sheet arrangement of the myocardium enables the atria & ventricles to contract in a coordinated & efficient manner.
Ø The myocardium is thickest at the Apex & thins out towards the base.
Ø This reflects the amount of work each chamber contributes to the pumping of blood.
Ø It is thickest in the left ventricle.
Ø The Atria & the ventricles are separated by a ring of fibrous tissue that doesn’t conduct electrical impulses.
ENDOCARDIUM: -
It forms the lining of the myocardium and the heart values.
Ø It is a thin, smooth, glistening membrane which permits smooth flow of blood inside the heart.
Ø It consists of flattened epithelial cells, continuous with the endothelium that lines the blood verses.
INTERIOR OF THE HEART:

The heart is divided into a right & left side by the septum, a partition consisting of myocardium covered by endocardium.
Ø After birth blood can’t cross the septum from one side to the other.
Ø Each side is divided by an Atrioventricular value into an upper chamber, the Atrium and a lower chamber the ventricle.
Ø The Atrioventricular values are formed by double folds of endocardium strengthened by a little fibrous tissue.
Ø The Retro ventricular value [Tricuspid value] has 3 flaps or cusps & the it atrioventricular value or Bicuspid has two cusps.
Ø The values between the atria & ventricles open & close passively according to change in pressure in the chambers.
Ø They open when the pressure in the Atria is greater than that in the ventricles.
Ø During ventricular systole (contraction) the pressure in the ventricles reissues above that in the Artia & the values snap that preventing backward flow of blood.
Ø The values are prevented from opening upwards into the atria by tendinous cords called ‘ Chordate tendons’ which expends from the inferior surface of the cusps to little projections of myocardium covered with endothelium called ‘papillary muscles’.

6. BLOOD SUPPLY

ARTERIAL SUPPLY


The right & left coronary oratories which branches from the aorta immediately distal to the aortic value.
VENOUS DRAINAGE:
The venous blood is collected into several small veins that join to from the coronary sinus which opens into the right Atrium.
7. NERVE SUPPLY:
PARASYMPHATHETIC N S:
The Vegas nerves supply mainly the SA & AV nodes and aerial muscles
Ø It reduces the Impulses & Decreases the heart rate
SYMPATHETIC N S:
It supplies the SA & AV nodes & the myocardium of Atria & Ventricles.
Ø Sympatyhic stimulation increase the rate & force of the heart beat.
8. FACTORS AFFECTING HEART RATE:
1. AUTOMATIC NERVOUS SYSTEM:
The rate at which the heart beat is a balance of sympathetic & parasympathetic activity.
2. CIRCULATING CHEMICALS:
The hormones Adrenaline & nor adrenaline secreted by the adrenal medulla, it increase the heart rate.
3. POSITION:
When the person is upright the heart rate is usually faster than when lying down.
4. EXERCISE:
Active muscles med more blood than resting muscles & this is achieved by an increased heart rate & selective vasodilatation.
5. EMOTIONAL STRESS:
During excitement fear or anxiety the heart rate is increased.
6. GENDER:
The heart rate is faster in women than men.
7. AGE:
In a babies & small children the heart rate is more rapid than in older children & adults.
8. TEMPERATURE:
The heart rate increases & decreases with body temperature.
9. BARORECEPTOR REFLEX:
These are nerve endings sensitive to pressure changes ( stretch) within the vessel situated in the Arch of the aorta & in the carotid sinuses.

CONDUCTIVE SYSTEM OF HEART

The components of the conductive system are :
1. S.A. node
2. A.V node
3. Inter nodal bundles
4. Bundle of His (right and left branch bundles)
5. Purkinjee fibres.

- The SA node is situated in the right atrium near the opening of superior venacava.
- The impulses originate from the AV node (situated on intraatrial septum).
- A.V node receives impulses from SA node and conducts it to the ventricle through the bundle of His., it starts from AV node and ramifies in the interventricular septum.
- The bundles of His gives Right & left branches, and passes to the right ventricle and to the left ventricles. They merge into purkinjee fibres.
Functions of conducting system:
1. Prevent overlapping of the atrial events with ventricular events(systolic)
2. Participates in syncytial nature of myocardium.
3. Initiates impulses rhythmically and automatically.
4. Conducts the impulse at a rapid rate.
The properties of the cardiac muscle are
1. Excitability and irritability .
2. Conductivity.
3. Contractility .
4. Rhythmicity and automaticity
5. Refractory period
6. Indefatigability.
7. Tonicity and
8. All or none phenomenon

Nutrition of the cardiac muscle:

1. ATP : (Adenosine triphosphate) energy for the heart is obtained by glycolysis and most of the energy by oxidation of glucose , lactate pyruvate, ketone bodies and aminoacids.
2. Oxygen : oxygen regulates oxidative processes for cardiac energy.
3. Sodium ion : it initiates and maintains the heart beat.
4. Calcium ion : it initiates and maintains the heart beat.
5. Potassium ion : it inhibits the contraction and prolongs the relaxation i.e., diastole
BLOOD VESSELS :



Blood circulates through the blood vessels.
They are arteries-which carries oxygenated (or) pure blood ,except the pulmonary arteries which carry de-oxygenated blood.
The veins carries de-oxygenated or impure blood except the pulmonary veins which carries pure blood from lungs to left atrium of the heart.
The arteries and veins are consists of three layers. They are
1. TUNICA ELASTICA, outer elastic layer made up of areolar connective tissue.it is thicker in veins than the arteries.
2. TUNICA MEDIA is made up of smooth muscle fibres, it is thicker in artery then the vein.
3. TUNICA INTIMA , is made up of endothelial cells ,and separated from middle layer by a membrane called elastic lamina.

The lumen in vein is narrower, while it is wide open in artery.
The veins are formed from smaller veins called venules and venous capillaries.
The veins collects the deoxygenated blood from lower limbs and other parts of the body and forms the inferior venacava , and they collect the impure blood from the upper limbs and head of the body and forms superior venacava and pour their contents into the right atrium of the heart.


PORTAL VEIN
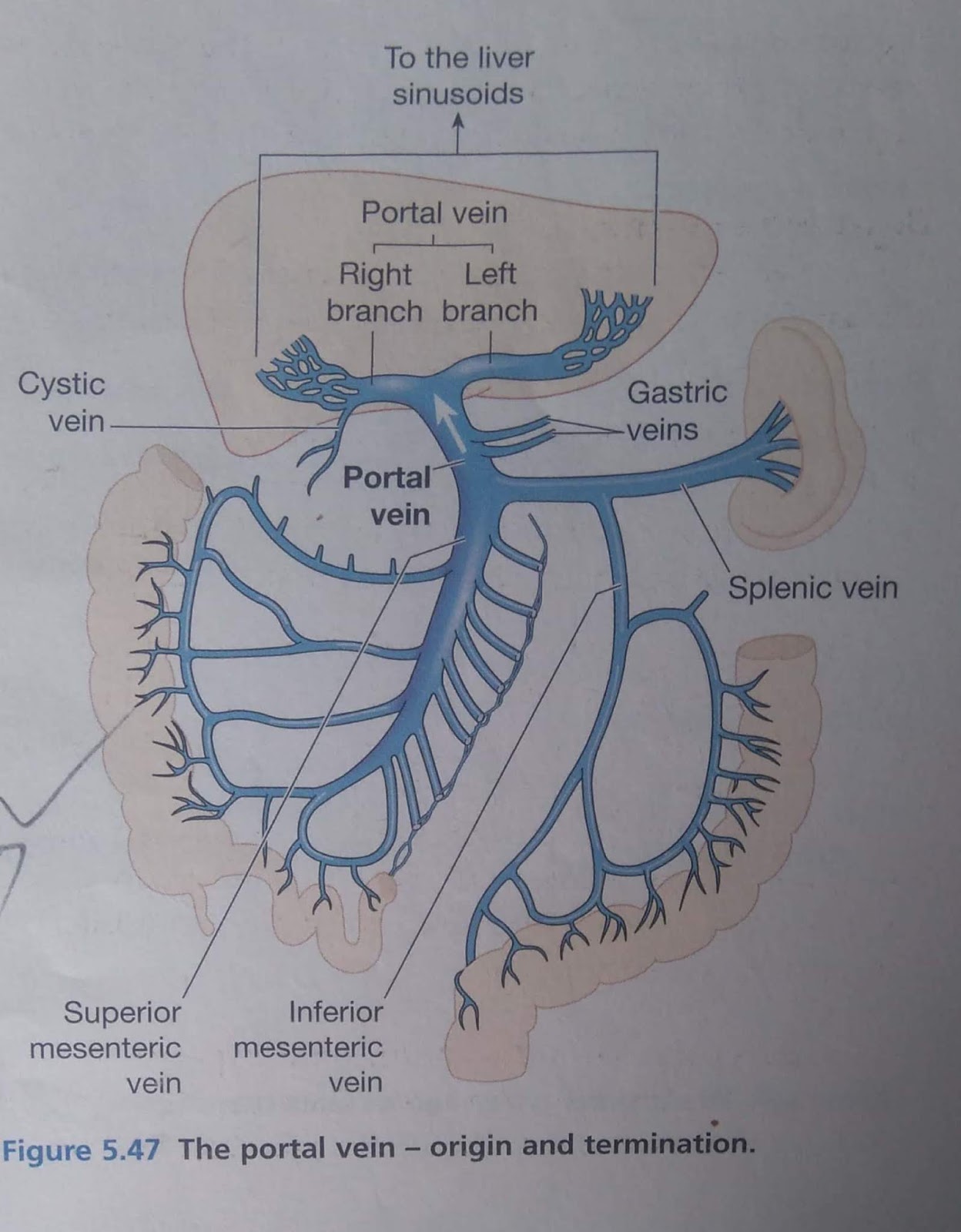
This is formed by the union of several veins each of which drains blood from the area supplied by the corresponding artery .
· The abdominal artery part of alimentary tract.
· The gall bladder
· The pancreas
· The spleen and conveys it to the liver.
· The portal vein breaks up into sinusoids which are drained by the hepatic veins into the inferior venecava.
· Portal vein begins in one set of capillaries and ends in another set of capillaries.
· The portal vein is about 8 cm long, it is formed by the union of superior mesenteric and splenic veins behind the neck of the pancreas.

· The portal veins ends at the right end of the porta hepatis by dividing into right and left branches which enter the liver.
1. The splenic vein ; it drains from the spleen, the pancreas and part of the stomach.
2. The inferior mesenteric vein returns the venous blood from the small intestine and the proximal parts of the large intestine, i.e. the caecum,ascending and transverse colon.it unites with the splenic vein to form thr portal vein.
3. The gastric veins drain from the stomach and the distal end of the oesophagus,then join the portal vein.
4. The cystic vein, which drains venous blood from the gall bladder, joins the portal vein.


ETIOLOGY


v Advice the patient to take rest after meal
BLOOD
Blood is a red –coloured, viscous fluid connective tissue
circulated in the body and is mainly composed of plasma and blood cells.
Physical characteristics of blood
v
Blood is composed of 45% of blood cells and 55%
of plasma.
Functions of blood
1.
Blood helps to transport the gases from lungs to
the tissues (o2) and from tissues to the lungs(co2).
2.
Blood helps to transport the absorbed digested
materials to the tissues of the body.
3.
Blood acts as a vehicle through which many
substances are transported to their places of activity.
4.
Blood helps to drain out waste materials present
in the body.
5.
Blood acts as a great defensive mechanisms.
6.
Blood helps to regulate body temperature.
7.
Blood maintains acid-base balance of the body.
8.
Blood has coagulation property due to which it
prevents loss of blood from the body.
9.
Blood helps to transport the hormones throught
the body.
ERYTHROCYTES/ RED BLOOD CELLS (RBC).
v
RBCs are small,circular,disc-shaped cells
suspended in the blood plasma.
v
All the cells in groups ,appear as red in colour
and thus blood becomes red-coloured.
v
RBCs are produced in the red bone marrow. The
process of formation of RBCs in the red bone marrow is called erythropoiesis.
v
Total lifespan of RBCs is 120days.
v
The RBCs contain a substance known as haemoglobin
and is enclosed in the stroma of RBCs
v
Haemoglobin is a complex protein of high
molecular weight.
v
Haemoglobin consists of a protein material
called globin and non-protein material called ‘haem’.
v
The haem contains iron which gives red colour to
the haemoglobin.
v
Haemoglobin (Hb)+oxygen(o2)=
oxyhaemoglobin(Hbo2).
v
Haemoglobin (hb)+Carbon dioxide
(Co2)=Carboxy-haemoglobin(HbCO2).
Normal values of RBCs/Erythrocytes.
1.
In adults -5 million/mm3 of blood.
2.
In male – 5 to 5.5 million/mm3 of blood
3.
In female – 4.5 to 5 million/mm3 of blood.
Functions of RBCs/Erythrocytes.
1.
It transports the gases such as o2 and Co2 in
the form of oxyhaemoglobin and carboxyhaemoglobin.
2.
It maintains acid-base balance by buffering
action of haemoglobin.
3.
RBCs help to maintain viscosity of blood.
4.
RBCs maintain iron balance of the body.
5.
Various pigments are derived from the
haemoglobin after disintegration of RBCs, e.g.bilirubin,biliverdin.
WBCS OR LEUKOCYTES.
The wbcs are colourless cells having,irregular shaped large
nucleus.
The normal count of leukocytes is 6000 to 10000/mm3 of
blood.
Classification of leukocytes(wbcs)
A.
GRANULOCYTES
They constitute about 75%. These contain granles in the
cytoplasm,hence called granulocytes.
1.
Neutrophils : the granules of these cells
are stained by neutral dye. The nuclei is many lobed.
Function : they ingest the microbes
and destroy it by phagocytosis.
2.
Basophils: the granules of these cells
are sustained by basic dye. The nucleus is usually oval or slightly
kidney-shaped .
Function : they are responsible for
destruction of products of antigen-antibody reactions.
3.
Eosinophils : the granules of these cells
are stained by red acidic dye called cosin. The nucleus is many lobed.
Function : phagocytosis.
B.
AGRANULOCYTES
These are mononuclear cells and they do not
show presence of granules in their cytoplasm.
1.
Monocytes : these are large cells with large
nucleus. The nucleus is convulted kidney –shaped.
Function : they give phagocytic action.
2.
Lymphocytes : these are produced in the lymph
glands hence called lymphocytes.
i.
Small lymphocytes : the thin rim is present
around nucleus and is stained by basic stains.
ii.
Large
lymphocytes: the nucleus is oval, rounded or kidney shaped and is stained by
basic stains.
Function : they are responsible
for the development of immunity against foreign substances such as
microorganisms.
Functions of leukocytes/WBCs.
v
Wbcs help in the process of phagocytosis.
v
Wbcs help in the formation of fibroblasts to
repair the areas of inflammation.
v
Wbcs give secretion of heparin which helps to
prevent intravascular clotting(thrombosis).
v
Wbcs prevent allergic reactions by
antihistaminic action.
v
Lymphocytes play an important role in the
production of antibodies.
Normal values :
1.
Erythrocytes (RBCs):
a.
Average : 5 million/mm3 of blood.
b.
In male : 5 to 5.5 million/mm3 of blood.
c.
In female : 4.5 to 5 million/mm3 of blood.
2.
Leukocytes (WBCs): 6000 to 10000/mm3 of blood.
3.
Thrombocytes (plateletus): 3to 4 lacs/mm3 of
blood.
4.
Haemoglobin :
a.
Average : 15gm/100 ml of blood.
b.
In male : 14 to 18 gm/100 ml of blood.
c.
In female : 12 to 16 gm/100 ml of blood.
Bleeding time : it is the time interval between moment at which the
blood starts bleeding to the moment at which the blood starts bleeding to the
moment at which it exactly stops.
Or
It is the time required for cessation of bleeding from a
small skin puncture.
Normal value:n1 to 3
minutes( by Dukes method).
Clotting time/ coagulation time : it is the time interval between the moment at which
blood escapes from the vessel to the moment at which clot is formed.
Normal value : 3to6 min (by Wrights capillary method).
Blood stream : it is the fluid remaining after formation of
clot.
BLOOD COAGULATION :
“When there is an injury to blood vessel, blood comes out
and within a few minutes,it losses its fluidity and forms a
red-coloured,semisolid jelly-like mass, i.e.clot. this process is known as
blood coagulation or blood clotting.”
Mechanism of blood coagulation/
process of blood clotting.
Step I
The injury to blood vessel leads to formation of a rough
surface. The platelets when come in contact with rough surface, they are
ruptured and thromboplastin is released. It is also released by damaged
tissues. This thromboplastin in the presence of calcium converts inactive
prothrombin present in the blood into active thrombin.
Prothrombin +thromboplastin +ca++-----> Thrombin .
Step II
The active thrombin converts inactive fibrinogen into
insoluble fibrin threads which form a network like structure .
Thrombin +fibrinogen ---------> Fibrin threads .
Step III
In the holes of these network of these fibrin threads the
blood cells get entangled to form a red-coloured semisolid jelly-like
mass,i.e.clot.
Thus ,the process of
blood coagulation completes.
Fibrin threads+Blood
cells ------> Clot .
Factors affecting /influencing blood coagulation.
a.
Factors Hastening/Accelerating/increasing blood
coagulation.
i.
Contacts of blood with rough surface and injury
to blood thrombocytes.
ii.
Temperature slightly excess than body
temperature may increase blood coagulation.
iii.
Excessive slowness of blood flow.
iv.
Snake venom.
v.
Presence of calcium salt.
vi.
Resting condition.
b.
Factors Hindering /retarding /preventing blood
coagulation .
i.
Contact with smooth surface .
ii.
Lowering body temperature
iii.
Removal of Ca++ ions from the blood by addition
of Na, K and citrate ions.
iv.
Presence of greasy material like oil, wax or
grease.
v.
Calcium deficiency in the blood.
vi.
Use of heparin.
PLASMA PROTEINS :
The number of
proteins present in the blood plasma are called plasma proteins,”. E.g. serum
albumin, serum globulin,prithrombin,fibrinogen.
Functions of plasma proteins :
i.
Plasma proteins maintain colloidal osmotic
pressure of the blood and help in regulating the distribution of fluid between
the blood and tissues of the body .
ii.
Prothromobin and fibrinogen are essential for
the blood clotting process.
iii.
Plasma proteins mainly globulins are responsible
for maintaining viscosity of blood which ultimately maintains the blood
pressure .
iv.
The plasma proteins act as a buffer which
maintain acid-base balance .
v.
Plasma proteins act as a store house of proteins
, from which the tissues can draw proteins during inadequate protein diet.
vi.
Plasma protein combine with certain substances
and help to carry them in bloodstream .
vii.
Plasma proteins helps in binding of drugs and
increase the duration of action of drugs .
viii.
Plasma globulins help in the formation of
antibodies which give protection against infection .
ABO BLOOD GROUP SYSTEM :
ABO blood group system was discovered by Karl Landsteiner in 1900.
i.
The blood of one person is not always compatible
with that of another person , hence before transfusion (donation ) of blood ,
it must be tasted or compatibility of acceptor’s blood is assured.
ii.
Only compatibility blood is to be transfused.
iii.
If incompitable blood is transfused then
agglutination of erythrocytes occurs which leads to haemolysis of transfused
blood cells (break downof RBCs).therefore, Rh+ve blood is not given to Rh-ve
persons.
iv.
There are four main blood groups.
Blood group A , blood group B,
blood group AB, blood group O.
Ø
Blood donor : a person who gives or donates
the blood to another person is known as blood donor.
Ø
Blood recipient/blood acceptor: A person
who requires or accepts the blood from another person is known as blood
acceptor.
Ø
Universal donor : A person who donates
the blood to all types of blood groups is known as universal donor.
Ø
Universal acceptor : A person who accepts
the blood from all the other blood groups is known as universal acceptor.
Ø
The membrane of erythrocytes contains antigens
called agglutinogens and people have natural antibodies in the plasma known as
agglutinins.
Ø
The agglutinogens are genetically determined and
are of two types i.e.’A’ and ‘B’.
Ø
The agglutinins in the plasma are of opposite
type.
Compatibility of blood groups (matching of blood groups)
Importance of blood group
i.
Blood group study has a great value in blood
transfusion.
ii.
Blood group study helps in the study of various
blood disorders.
iii.
Blood group study is useful in forensic
medicines.
iv.
Blood group study is helpful in experimental
purposes.
RH FACTOR :
It is an agglutinogen(antigen)
of “rhesus monkey”.
Apart from antigen ‘A’ and antigen ‘B’ about 80to 90% of the
people contain one or more antigens on the membranes of RBCs called Rh-antigen
or Rhesus factor.
If Rh factor is present in the persons blood then blood group
is described as Rh+ve and if Rh factor is absent in the persons blood then
blood group is described as Rh-ve.
Significance /importance of Rh factor.
i.
Rh factor has a great value in blood transfusion
because transfusion of Rh+ve blood to Rh-ve person stimulates the immune
response which causes haemolysis of transfused blood cells.
ii.
Rh factor is helpful in detecting the blood
group of child by considering father’s and mother’s blood group study.
THRPMBOSIS :
The process of formation of blood clot inside the blood
vessel which may block the blood circulation is known as thrombosis.
The clot which is formed inside the blood vessel is known as
“thrombus”. Thrombosis may be caused because of slow blood flow or infection to
inner side of the blood vessels.
Embolism :
The process of formation of embolus in the bloodstream which blocks the blood
circulation is known as embolism.
The embolus may be bubble of air or in some cases blood clot
or debris particle.
Phagocytosis :
The process in which the cell engulfs or ingests the
microbes,foreign particles and digests or destroys them within the cell is
called phagocytosis, e.g. neutrophils and monocytes actively show phagocytic
action.
Haemolysis :
Haemolysis means
breakdown of RBCs.
The haemoglobin comes into the plasma after breakdown of
RBCs. This phenomenon is known as laking of blood.
Fibrinolysis :
The process of
breakdown of fibrin threads within the clot by the action of proteolytic
enzymes is known as fibrinolysis.
Blood disorders :
1.
ANAEMIA :
Anaemia means decrease in number of RBCs in
the blood, or decrease in percentage of haemoglobin in the blood.
Causes :
i.
Excessive loss of blood.
ii.
Failure of function of red bone marrow to
produce RBCs.
iii.
Destruction of RBCs by haemolysis.
iv.
Deficiency of iron in the body
v.
Defective formation of RBCs.
TYPES OF ANAEMIA :
a.
Pernicious anaemia
b.
Megaloblastic anaemia
c.
Microcytic anaemia
d.
Sickle cell anaemia
e.
Iron deficiency anaemia.
2.
Polycythemia :
“it means an abnormal increase in RBCs in
the blood”. In this condition the skin and mucous membranes of the mouth are
red and conjunctiva is also red.
3.
Leukaemia :
“ leukaemia means uncontrolled increase in
production of WBCs in the blood”. It is also called as cancer of blood.
4.
Leucopenia :
“leucopenia means the condition in which
there is a decrease in number of WBCs below 4000/mm3 of blood”.
5.
Leukocytosis :
The condition in which the number of
circulating leukocytes increases in the blood circulation.
Pathological leukocytes occurs when a blood
leukocyte count is above 11,000/mm3 of blood.
6.
Haemophilia :
a.
It is the condition in which bleeding occurs
continuously even with a minor injury or a cut.
b.
In this case blood does not clot
c.
It is a hereditary disease which runs in the
families.
7.
Erythroblastosis foetails :
It means the death of the foetus due to mass
destruction of its red cells when their Rh-ve blood happens to receive Rhesus
antibodies from the blood of mother .
ANGINA PECTORIS

Angina pectoris is a pain in the chest caused by myocardial ischemia .
Ischemia means deficiency of blood supply to the myocardium.

ETIOLOGY
§ Blockage or narrowing of a coronary artery
§ Cigarette smoking
§ Exposure to cold or heat
§ Myocardial ischemia
§ Lack of oxygen
CLINICAL MANIFESTATION

§ Chest pain
§ Tachycardia
§ Increased or decreased blood pressure
§ Dyspnea
§ Nausea
§ Vomiting
§ The pain lasts for 5 to 10 minutes
TYPES OF ANGINA

There are 7 types
1.stable angina :
It is characterized by pain and discomfort caused by emotions,physical exertion etc.
2.Unstable angina :
It occurs mostly in night ,pain more than 20 minutes can relived by medical treatment
3. variant angina :
Pain takes more longer time . it may can occur when patient take rest also.
4. Noctural angina :
It assosciated with rapid eye movement sleep during dreaming .
5. Angina decubitus :
Pain occur when patient sits or stand up.
6.Intractable angina :
It is a chronic pain in the chest .
7.Post infraction angina :
It occur the pain after myocardial infarction .
DIAGNOSTIC EVALUATION
o Chest X-ray
o ECG
o Tread mill test
o Echocardiography
o Increased creative protein (CRP)
MEDICAL MANAGEMENT
· Nitrates this help to relive pain such as nitroglycerine tablets
· Antianginal help to relieve pain and discomfort . example Beta blockers
· Calcium channel blockers it prevents vasodilation of coronary arteries . Example : diltiazem ,folodipine .
· Morphine it acts as an analgesic and sadatives .
· Anti platelet therapy it helps to reduce the coronary artery disease and clot formation.
· Aspirin helps to promote normal blood flow
· Oxygen supply
SURGICAL MANAGEMENT :
ü LASER ANGIOPLASTY
It is performed with a catheter containing fibers that carry laser energy. This laser energy used to dissolve the blockage in the coronary artery.
NURSING MANAGEMENT :
v Cardiac monitoring with 12 leads ECG.
v Assess the level duration of pain
v Assess signs and symptoms
v Check the vital signs
v Advice the patient to do some exercises
v Advice the patient to have small and frequent meals
v Advice the patient to stop smoking
v Advice the patient to take rest after meal
v Advice the patient to take food high in fiber because it prevents the constipation .


MYOCARDITIS

Inflammation of the myocardial wall.

ETIOLOGY :
· Viruses
· Bacteria
· Fungi
· Parasites
· Radiation

· Pharmacological factors : drug such as lithium , cocaine
· Chemical factors
· Toxic agents such as lead
· Connective tissue disease .
CLINICAL MANIFESTATION :
§ Fever
§ Malaise
§ Fatigue
§ Dyspnea
§ Pharyngitis
§ Nausea and vomiting
§ Chest pain .
DIAGNOSTIC EVALUATION :
v ECG
v Laboratory test (examination )
v Myocardial biopsy
v Echocardiography
v Gallium scan
v Chest X-ray .
MANAGEMENT :
§ Digoxin to treat ventricular failure
§ Oxygen therapy
§ Provide bed rest
§ Restricted activity
§ Immune suppressive therapy such as prednisone,cyclosprin.
§ Medication such as –
Diuretics
Vein and orbital dilator
Intrope
Angiotensin inhibitor .
NURSING MANAGEMENT :
v Decrease cardiac output is an ongoing nursing diagnosis in the care of the patient with myocarditis .
v Assess for the sign and symptoms of congestive heart failure
v Decrease cardiac work load
v Prescribed medications that increase the heart contractility.
v Careful monitoring and evaluation of patient taking these medications are necessary .
v Nurse should assess the level of anxiety and help the patient to reduce anxiety .
v Care include monitoring for the complications and providing .


%20d%20trans.jpg)





{kind=link}
0 Comments